A Guide to Physical Disabilities and Inclusion
Throughout history, many social and cultural majorities have tended to reject, isolate, and exclude those with physical disabilities and different needs. The Greeks and Romans would habitually abandon, or murder, children who did not ‘fit in’; the Tudors could find no value in the ‘helpless poor’; and the Victorians allowed many children with disfigurements to become circus exhibits. More enlightened and inclusive practices can certainly be found in 21st-century educational settings, but change has rarely kept pace with aspirations.
Diverse physical disabilities and needs
Though an individual’s needs will always be specific and personal, Frederickson and Cline1 propose three useful categories of physical needs which mainstream educators may find useful when thinking about aspects of their own provision:
- Severe physical disabilities: which include motor impairments associated with medical conditions such as cerebral palsy. These in turn can further influence many other aspects of child development.
- Dyspraxia and development coordination disorder (DCD): can cause impaired motor coordination even when there is no underlying medical condition. Developmental delays are common – a feature which has broad implications for social development and educational advances.
- Chronic and severe illness: because medical needs are prioritised, educational attendance and progress are disturbed. In addition, a child’s symptoms may impose limits on what can be achieved in a classroom setting.
Disability and education: the historical perspective
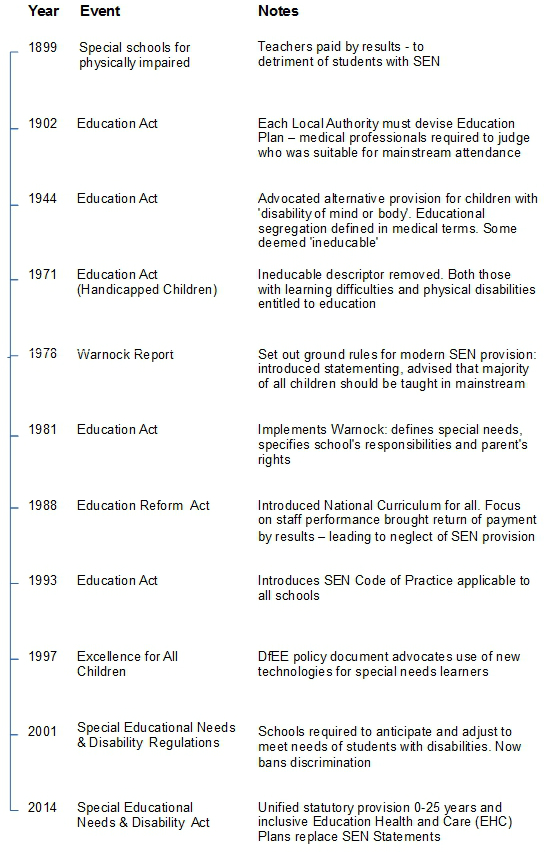
For children with physical needs, the journey towards inclusion has been a hard road – for example, the first UK educational provision for those with disabilities came into being little more than one hundred years ago. The timeline below will help to track the progress of this reform by noting some relevant milestones:

Redefining physical disabilities
According to the ‘World Report on Disability’2, disability is ‘an evolving concept’, and the most significant driver in terms of equal status for those with disabilities has been the transition from defining disability exclusively in medical terms towards an awareness of the social dimension as it impacts upon individuals. As a consequence, many living with impairments refuse to acknowledge the notion of ‘disability’, pointing out that their exclusion – from educational institutions, for example – is solely the result of society’s barriers to access. Recent disability legislation has begun to acknowledge this ‘social model‘ of disability. For instance, the 2005 Disability Discrimination Act3 imposes ‘general’ duties on public bodies, which include the following:
- To promote equality of opportunity between disabled people and other people;
- To eliminate harassment of disabled people that is related to their disability;
- To promote positive attitudes towards disabled people;
- To … take account of disabled people’s disabilities, even where that involves treating a disabled person more favourably …
In addition, the Act also requires the execution of ‘specific’ duties, including:
- Developing and publishing a Disability Equality Scheme …
- Publishing an Annual Report on progress and activities;
- … involving disabled people in all aspects of the Scheme’s development and implementation.
Attitudes in transition
Disability awareness has, of course, influenced attitudes and practices in the educational world too. Devarakonda4, for instance, reports that many research findings confirm ‘teachers’ attitudes change from negative to positive as a result of their experiences with children with disabilities’.This can be tracked via research initiatives, such as the survey information below adapted from Frederickson and Cline. This data traces the development of the teaching profession’s attitudes towards educational provision for children with physical disabilities :
Year: 2000
Croll and Moses5 (2000)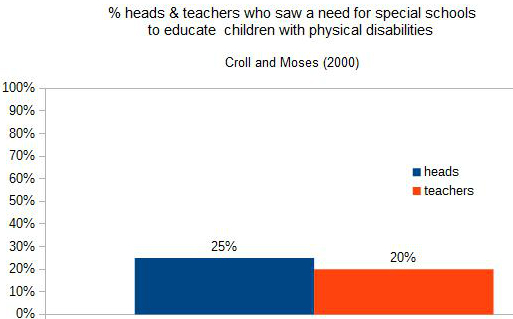
Year: 2005
Bloom6 (2005)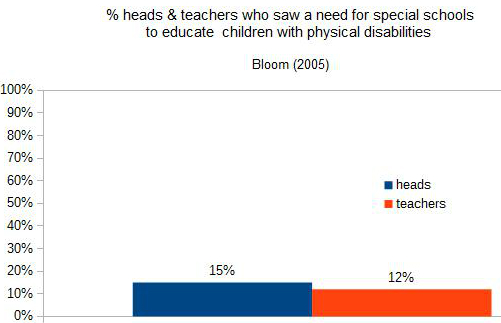


As regards the issue of educational segregation, Fontana7 has identified precisely why this initiative consistently failed to achieve its primary aims:
‘One of the problems of special schools, no matter how good, is that children become labelled, in their own eyes as well as in those of adults and other children, as being “different” … in an undesirable way. This kind of stigma places additional burdens upon children and their parents.’
He also points out the underlying irony, adding, ‘the purpose of such education after all is to enhance children and not to handicap them further.’
Thankfully, as the data above confirms, the tide is now turning, and Devarakonda has noted research listing several specific areas of improvement, such as:
- newly qualified and younger teachers show positive attitudes towards inclusion…
- teachers who are satisfied with the support available, and the development and training they have undergone, develop a positive attitude towards inclusion;
- teachers from mainstream schools perceived that inclusion resulted in a positive impact on the children without disabilities.
Read more about disability and inclusion here in our article: Disability and Inclusion: Making the Outdoors Accessible for Everyone
Mainstream inclusive practice
When considering the prospect of making children with physical needs feel welcome in mainstream settings, four principal areas are consistently mentioned:
1. Access to the educational institution
Apart from physical access to buildings, classrooms and facilities, other issues such as appropriate pain relief, and ensuring that each teacher’s mode of delivery does not disadvantage those with impairments, must all be carefully evaluated.
2. Keeping staff informed of children’s needs
Teachers may not always readily appreciate the nature and consequences of a physical disability. Keeping staff informed about a child’s impairment is a courtesy which helps them: liaise with parents and other professionals, better assess the impact and benefits of educational initiatives, and better understand the burden of impairment for the child.
3. Delivering a broad and balanced curriculum for all
For children with disabilities, one of the perceived advantages of mainstream settings is better access to a broad and balanced curriculum. However, it is still too common to find that this is just not the case. The worst forms of tokenism once had children copying, developing handwriting, and making craft items as a pale substitute for educational advancement. Whilst accepting progress has been made, Science, PE and Games perhaps still have some ground to make up in this respect.
However, some PE and Games initiatives have sought to boost the move towards greater inclusion. For example, though the age disparities prevent absolute comparison, the Sport England data on a whole range of school sports shows not only the difference between the preferences of young people with disabilities and those of total school populations, but also some useful points of correlation such as the mutual popularity of swimming, gym and football – as depicted in the extracts below which shows the 1 to 5 rankings and percentages for the most-favoured activities:
a) School sport preferences – disabled population
Sport England8 (2001)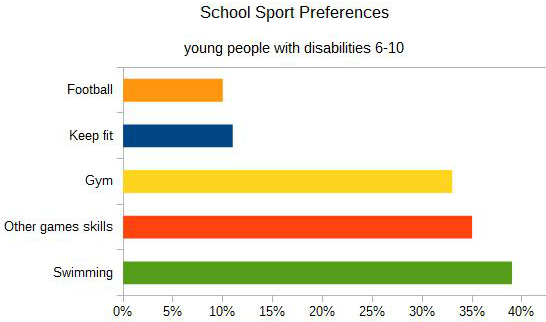
a) School sport preferences – whole population
Sport England (2001)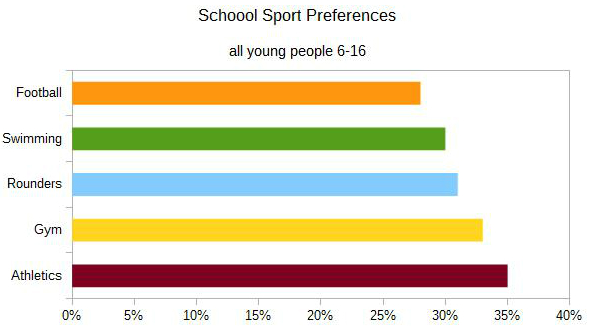


4. Accommodating illness and medical needs
Some children could attend a mainstream setting if only their medical needs (e.g. treatment and/or medication) could be properly met. Even though schools have historically contributed enormously to overall child health and well-being, the differentiated support needed to transform the life chances of individuals has too often lagged behind. Similarly, when a child has to cope with longer-term illness and the resultant planned and unplanned absences, institutions can sometimes find it very difficult to provide adequate and effective support – a failing which can only be addressed at a strategic level.
Mapping an inclusive future
Many SEN commentators mention the Italian Reggio Emilia preschools as aspirational models of best practice. Here, according to many, the pedagogy of an inclusive community seems to accept Reid and Valle’s9 observation that differing physical needs should be seen as ‘human variation rather than pathology’.
A few of Nurse’s10 observations of Reggio Emilia (in 2001) are quoted in conclusion and clearly identify some areas where Italian inclusive practice is indeed highly nuanced and exemplary:
‘… the preschools minimise the effects of disability and a slower rate of learning because the learning environment matches the developmental and social needs of the individual child … A difference between the system in the UK and the Reggio response is the commitment to children learning as a group, from each other … Reggio Emilia is a stable, prosperous and cohesive community. The preschools are a highly regarded part of that community which in turn values the group experience they offer to young children. Provision is local so the children are not placed in distant centres which isolate them and their families from their own community.’ [References]